심폐 소생술-2, Cardiopulmonary resuscitation(CPR)-2

응급 기본 심폐 소생술 처치
표 41. 생명을 유지하기 위해 기본 심폐 소생술을 한다.
| 기본 심폐소생술의 순서 |
|
출처와 참조문헌; Manual of emergency pediatrics 5th edition, Robert M. Reece, M.D., p.20
- 호흡 정지 상태에 있는지, 쇼크 상태에 있는지, 심장 정지와 호흡 정지의 상태에 있는지 속히 평가하고 알아야 한다.
- 그럼 얼마나 속히 알아야 하나. 30초~1분 내 생명을 유지하기 위한 기본 심폐 소생술 응급처치나 전문 심폐 소생술 응급처치를 하지 않으면 생명을 구할 수 없다.
- 공기가 유통할 수 있게 기도가 열려 있는지 그렇지 않으면 기도가 막혀 있는지 알아본다. 가능한 안전한 장소로 환아를 옮기고 등을 바닥에 대고 반듯이 눕힌다.
- 가능하면 입안이나 비강 내에 있는 분비물을 흡입해서 빨아낸다([부모도 반의사가 되어야 한다-소아가정간호백과]-제21권 소아청소년 가정 학교간호-흡입구 참조).
- 다음 상태를 체크한다.
- 숨을 그렁그렁 쉬는지,
- 콧날개(콧방울/비익)가 숨 쉴 때마다 벌렁벌렁 거리는지,
- 앞가슴이나 복부가 숨 쉬는 대로 올라갔다가 내려오는지,
- 갈비뼈 사이이의 근육이 흉강 속으로 빨려 들어갔다 나오는지,
- 호흡수는 얼마인지,
- 콧구멍 근처에 처치자의 귀를 바싹 갖다 댔을 때 공기가 폐에서 나왔다 들어가는 소리가 나는지 등을 체크해야 한다.
- 숨을 쉬는지,
- 호흡곤란이 있는지,
- 호흡이 정지됐는지 알아보아야 한다.
- 맥박이 뛰는지, 맥박 수, 맥박이 강한지 맥박이 느린지, 또는 불규칙적으로 뛰는지 맥박을 짚어본다.
- 피부의 색이 창백한지 푸른지, 피부가 찬지 따뜻한지 등을 검사해서 혈액 순환 상태를 알아본다. [부모도 반의사가 되어야 한다-소아가정간호백과]-제1권 소아청소년 응급의료 참조.
- 그 환자의 의식 청명도가 어느 정도인지 알아본다. 민활한지, 말에 반응하는지, 외부에서 가한 아픈 자극에 반응하는지, 그런 자극에 아무 반응이 없는지 등으로 의식 청명도를 빨리 알아본다.
- 호흡 정지와 심장 정지가 생기게 한 원인을 찾고 심폐 소생술을 하기 위해 옷을 전부 벗긴다. 그리고 외상이 있는지 몸에 어떤 징후가 있는지 알아본다.
- 호흡 정지와 심장 정지가 기도 폐쇄로 생겼는지, 기도의 통기 문제로 생겼는지, 또는 다른 문제로 생겼는지 순식간에 알아봐야 한다.
- 이상 설명한 1~10까지 증상 징후 등을 30초 내, 적어도 1분 내 알아보고, 그 다음 필요한 처치를 시작해야 한다.
- 이런 제반 문제를 30~60초 내 알아본다는 것은 의사들에게도 쉬운 일이 아니다. 또한 30~60초 내 그런 정보를 다 알아낸 다는 것은 비의료인 부모들에게는 더군다나 어려운 일이다.
- 생명을 구출할 수도 있고 구출할 수 없다는 찰나에 서있다는 사실도 알아야 한다.
- 생명 구출에 관한 그런 정보를 평소에 더 많이 더 확실히 배워 알고 있으면 생명을 유지하기 위한 기본 심폐 소생술을 하는데 보다 더 효과적으로 할 수 있다.
다음과 같이 생명 유지 기본 심폐 소생술을 시작한다.
- 이상 설명한 1~10항을 체크한 결과를 1분 내에 종합해서 호흡 정지와 심장 정지가 생겼다고 판단을 하면 생명 유지를 기본 심폐 소생술을 다음과 같은 순서로 하는 것이 보통이다.
- 호흡 정지와 심장 정지가 있다는 것을 확인하고
- 기본 심폐 소생술이나 전문 심폐 소생술을 혼자서 적절히 하기가 어렵다.
- 때문에 도와줄 수 있는 사람을 크게 소리 내어 불러 도움을 청한다.
- 가능하면 그와 동시에 의사, 구급대원, 응급실, 구급차 등의 도움을 긴급히 전화로 청한다.
- 그와 동시에 기본 심폐 소생술에 가장 적절한 체위를 유지하기 위해서 환아의 등을 바닥에 대고 안전한 장소에 눕힌다.
- 환아의 얼굴을 살짝 옆으로 돌리고 턱을 살짝 위쪽으로 올려서 기도가 열리게 한다. 이 때 목에 어떤 이상이 있거나 외상이 있을 때는 의사의 지시가 없이 목을 함부로 돌리지도 말고 밀지도 끌지도 비틀어서도 안 된다.
- 처치자의 귀를 환아의 입이나 코에 바싹 대고 숨소리가 들리는지 공기가 숨통(기도) 속으로 들어갔다 나갔다 하는지 호흡이 정지 상태에 있는지 재확인 한다.
- 호흡 정지 상태에 있다는 것을 확인한 후 처치자의 입을 환아의 입에 대거나 코에 대거나, 또는 입과 코, 두 곳에 대고 공기를 환아의 기도 속으로 맨 처음 2번 불어넣는다.
- 이 때 보통 때 숨 쉬는 것과 같이 앞가슴이 위쪽으로 올라오는지 안 올라오는지 확인한다.
- 환아의 기도가 이물 등으로 완전히 막혔을 때는 처치자가 불어넣은 공기가 막힌 기도 때문에 폐 속으로 들어갈 수 없으므로 앞가슴이 위쪽으로 올라가지 않는 것이 보통이다.
- 나이에 따라 적절한 신체 부위에서 맥박을 짚어 심장이 뛰는지, 또는 뛰지 않는지를 확인한다.
- 1세 이전 영아나 작은 유아를 위해 인공호흡을 할 때는 처치자의 입을 환아의 입과 코, 두 부위에 대고 인공호흡을 하고,
- 1세 이후 유아나 학령기 소아를 위해 인공호흡을 할 때는 처치자의 입을 환아의 입에만 대고 비익(콧방울)을 손가락으로 눌러 양 쪽 콧구멍을 막고 인공호흡을 시작한다.
- 그와 동시에 심장마사지(심장 압박)를 시작한다.
- 전문 심폐 소생술을 효과적으로 할 수 있는 의료기구가 있을 때는 인공호흡기로 인공호흡을 하고,
- 인공호흡 백(호흡 주머니)과 마스크 등을 이용해서 인공호흡을 한다.
- 여기서는 전문 인명소생술에 관한 더 자세한 설명은 생략한다.
- 1세 이전 영아들과 8세 이전의 유아들과 소아들에게 심폐 소생술을 할 때 1분에 20번 인공호흡을 하고 1분에 100번 심장마사지를 한다.
- 1세 이전 영아의 기도가 이물로 막혀 호흡이 정지되고 심장이 정지됐을 때는 기본심폐 소생술을 하면서 양 어깨 사이 등 부분을 손바닥으로 5번 연거푸 쳐서 기도 속 이물을 빼주던지
- 앞가슴 밀기 기도 속 이물제거 처치로 해서 기도 속 이물을 빼준다.
- 1~8세 유아나 학령기 아이들의 기도가 이물로 막혀 호흡이 정지되고 심장이 정지됐을 때는 심와부(오목가슴)를 손바닥으로 5번 흉곽강 속쪽을 향해 밀어서 기도 속 이물을 빼준다.
- 1세 이상 유아나 학령기 아이의 기도 속에 이물이 들어갔을 때 의식이 있으면 하임리크 처치법이나 심와부(오목 가슴) 밀기로 기도 속 이물을 빼줄 수 있다(기도 이물 질식 사진 참조).
- 생명 유지를 위한 기본 심폐 소생술을 얼마나 오랫동안 해야 되는지 확실하게 말할 수 없다.
- 호흡 정지와 심장 정지를 일으킨 원인에 따라 산소호흡 치료 등 다른 종류의 치료 방법으로 하는 전문 심폐 소생술을 요하는 것이 보통이다.
- 생명 유지를 위한 기본 심폐 소생술도 가능하면 의사의 응급전화 치료지시에 따라 하는 것이 가장 이상적이다.
| 5번 기본 심장마사지를 하고 1번 인공호흡을 하는 것이 보통이다(도표 42 참조). |
출처 및 참조 문헌
- Robert M. Reece, Manual Emergency Pediatrics, 4th Ed. p8
- Choking/ CPR. AAP
심폐 소생술을 할 때 더 알아야 할 몇 가지 사항
- 기본 인공호흡을 할 때 환아의 나이와 입의 크기에 따라 처치자의 입을 환아의 입에만 대고 할 것인가, 처치자의 입을 환아의 입과 콧구멍 두 부위에 대고 할 것인가를 결정한다.
- 여기서는 환아가 갑자기 숨을 쉬지 못하거나 거의 쉬지 못할 때 처치자의 입을 환아의 입에 대고 또는 입과 콧구멍 두 부위에 대고 환아의 기도 속에 공기를 직접 불어넣어 환아의 폐 속에 산소를 공급하는 인공호흡 방법과 심장 마사지(흉부 압박 테크닉)를 하는 방법에 대해 설명한다.
- 인공호흡과 심장 마사지 둘 중 인공호흡을 먼저 해서 환아에게 산소 공급을 하는 일이 우선적이고, 또 인공호흡을 시작하기 전에 기도 속을 열어주어야 공기가 기도를 통해서 잘 유통된다.
- 만일 기도가 완전히 막혔을 경우 처치자가 공기를 환아에게 인공호흡을 통해서 불어넣어도 공기가 숨통(기도)을 통과해서 환아의 폐 속으로 들어갈 수가 없다.
- 감염병으로 인해 호흡 정지와 심장 정지가 생길 수 있다.
- 감염병으로 호흡 정지와 심장 정지가 생긴 환아의 생명유지를 위해 기본 심폐 소생술을 했던 처치자가 환아로부터 세균에 감염될 수 있다. 기본심폐 소생술을 한 후 처치자는 의사의 권장에 따라 적절한 예방적 항생제 치료를 받아야 한다.
- 영아 돌연사로 호흡 정지와 심장 정지가 있는 영아를 발견했을 때는 가능한 한 전문 심폐 소생술을 할 수 있는 병원으로 후송할 때까지 기본 심폐 소생술을 계속 하는 것을 권장한다.
- 의식이 없고 호흡이 정지되고 심장이 정지된 환아의 입 안 이물질이 보이면 그 이물질을 손가락으로, 또는 적절한 의료기구로 꺼내는 처치를 권장한다.
- 주의할 것은 인두강 속 이물질이 다음에 있는 하 기도 속으로 더 깊숙이 들어가서 아래에 있는 기도가 더 완전히 막힐 수 있다는 것이다(기도 속에 이물이 들어갔을 때 참조).
- 나이에 따라 소아청소년 기본 심폐 소생술을 할 때 입에다 처치자의 입을 대고, 또는 환아의 입과 코에다 처치자의 입을 대고 하는 인공호흡을 사진으로 보기
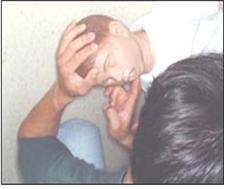
사진 245. 1. 처치자의 귀를 환아의 입이나 콧구멍에 바짝 갖다 대고 환아가 숨을 쉬고 있는지 알아본다.
Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP

사진 246. 2. 앞가슴이나 복부가 숨 쉬는 대로 올라갔다 내려갔다 움직이는지 관찰하든지 환아의 앞가슴 위에 처치자의 손을 올려놓고 숨 쉬는지 알아본다.
Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP

사진 247. 3. 목에서 경동맥을 재고 있다.
1세 이하면 영아의 팔에 있는 상완동맥이나 서혜부에 있는 대퇴동맥에서 맥이 뛰는지 알아보든지, 1세 이상 된 유아나 학령기 아이면 목에 있는 경동맥 맥을 짚어 심장이 뛰는지 알아보는 것이 보통이다.
또는 가슴에서 심장이 뛰는지 알아 볼 수도 있다. 이렇게 알아보는 데 1~2초 이상 더 걸려서는 안 된다. 평소에 맥박을 짚는 법을 배운다.
Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP

사진 248. 4. 상완동맥을 재고 있다.
1~2초 내에 목이나 팔이나 서혜부에서 맥이 뛰는지 또는 가슴에서 심장이 뛰는지 알아본다.
Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP

사진 249. 5. 대퇴동맥에서 맥박을 재고 있다
1~2초 내에 목이나 팔이나 서혜부에서 맥이 뛰는지 또는 가슴에서 심장이 뛰는지 알아본다.
Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP

사진 250. 6. 또 다시, 가슴에서 심장이 뛰는지 숨을 쉬는지 알아본다.
또는 목이나 팔이나 서혜부에서 맥이 뛰는지 안 뛰는지 알아본다.
Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP

사진 251. 7. 기도가 열려 통기가 되고 숨을 잘 쉬도록 한다.
처치자의 한쪽 손을 이마에 올려놓고 환아의 머리를 뒤로 살짝 젖히고 얼굴과 머리를 옆으로 살짝 젖힌 다음 다른 손으로 턱과 얼굴을 살짝 추켜올린다.
Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
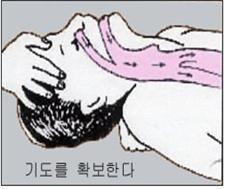
사진 252. 8. 목을 뒤로 살짝 젖힌다.
이렇게 처치하는 목적은 사진과 같이 인공호흡을 할 때 공기가 기도 속으로 잘 들어가도록 하기 위해서이다 이런 처치법을 기도확보라고 한다.
Copyrightⓒ 2011 John Sangwon Lee, MD., FAAP

사진 253. 9. 입안이나 비강 속에 분비물이 있으면 분비물을 제거한다.
여기까지 처치하는데 소요되는 시간이 30초 이상 더 걸려서는 안 된다. 다음은 처치자의 입으로 공기를 환아의 입이나 입과 콧구멍 속을 통해 기도 속으로 불어넣는다. 맨 처음에는 2번 기도 속으로 공기를 불어넣으면서 보통 때 숨 쉴 때와 같이 앞가슴이 위로 올라오는지 관찰한다. 만일 기도가 완전히 막히면 공기가 폐 속으로 들어갈 수 없기 때문에 공기를 불어넣을 때 앞가슴이 위쪽으로 올라오지 않는 것이 보통이다.
Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP

사진 254. 10. 처치자의 입을 1세 이하의 영아나 작은 유아의 입과 콧구멍에 동시에 대고 공기를 기도 속에 불어넣는다. 1세 이상 되는 유아나 학령기 아이를 위해서 입으로 인공호흡을 할 때는 코 날개를 눌러 콧구멍을 손가락으로 막고 처치자의 입을 환아의 입에 대고 인공호흡을 시작한다.
Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP

사진 255. 11. 1세 이상 큰 유아에게 기본 심폐 소생술을 할 때는 처치자의 입을 유아나 학령기 아이의 입에 대고 공기를 기도 속에 불어넣는다. 이 때 한 손으로 콧구멍을 막는다.
Copyrightⓒ 2011 John Sangwon Lee, MD., FAAP

사진 256. 12. 한 처치자는 처치자의 입을 환아의 입에만, 또는 입과 콧구멍, 두 부위에 대고 공기를 기도 속에 불어넣고 다른 처치자는 심장 마사지를 해서 기본 심폐 소생술을 한다.
Copyrightⓒ 2011 John Sangwon Lee, MD., FAAP
입으로 하는 인공호흡
- 구조자(처치자)가 환아의 입이나 콧구멍 근처에 귀를 바짝 갖다 대고 아이가 숨을 쉬고 있는지, 앞가슴이나 복부가 숨 쉬는 대로 위쪽으로 올라갔다 아래쪽으로 내려갔다 움직이는지 관찰하든지, 환아의 앞가슴 위에 처치자의 손을 올려놓고 숨 쉬는지 또는 숨을 쉬지 않는지 알아본다.
- 환아가 숨을 거의 쉬지 못하거나, 전혀 숨을 쉬지 않는다고 판단됐을 때는 다음과 같이 기본 심폐 소생술을 즉시 시작한다.
- 우선 공기가 콧구멍→비강, 입안, 인두→ 후두→ 기관→ 기관지 속을 통해 폐포 속으로 들어갈 수 있도록 기도를 열어준다. 이런 처치를 기도 확보라 한다.
- 한쪽 손을 환아의 이마 위에 올려놓고 머리를 뒤로 살짝 젖히고 다른 쪽 손을 그 환아의 턱 밑에 대고 턱을 살짝 위로 추켜올려 인두 속 기도 부분이 크게 열리게 하고 후두, 기관, 기관지 등 기도가 활짝 열리도록 한다.
- 이 때 혓바닥과 혀뿌리가 인두강 속 뒤로 당겨 들어가 인두 기도 부분이 막히지 않도록 주의한다.
- 가능한 한 인공호흡을 하는 동안, 머리, 얼굴, 목을 이런 위치로 계속 유지시킨다.
- 그렇지만 목뼈가 손상됐거나, 손상됐다고 의심될 때는 목을 함부로 움직여서는 절대로 안 된다.
- 환아의 크기와 나이에 따라, 처치자의 입을 환자의 입에만, 또는 입과 콧구멍 두 부위에 대고 인공호흡을 해야 한다.
- 병원에서 심폐 소생술을 시작할 때까지, 또는 기본 심폐 소생술을 더 이상 할 필요가 없다고 판단될 때까지 계속 기본 심폐 소생술을 한다.
- 신생아나 영아와 같이 체구가 작은 환아를 위해 기본 심폐 소생술을 할 때는 신생아나 영아의 입과 콧구멍 두 부위에 처치자의 입을 대고 공기를 불어넣는다.
- 인공호흡을 해 주는 처치자도 환아의 나이와 크기에 따라 적당한 량의 공기를 흡인한 후 처치자가 입을 크게 벌리고 신생아나 영아의 입과 콧구멍 두 부위를 통해 공기를 기도 속으로 불어넣어야 한다.
- 돌 이후 유아나 학령기 아이에게 인공호흡을 할 때는 그 환아의 양쪽 코 날개(콧방울)를 처치자의 두 손가락으로 꼭 쥐어 양쪽 콧구멍을 막고 처치자의 입을 그 환아의 입에다 꼭 대고 그 환아의 입을 통해 공기를 기도 속으로 불어넣는다.
- 보통 때 숨 쉴 때처럼 환아의 앞가슴이 올라갔다 내려갔다 하도록 처치자는 적당한 양의 공기를 흡입한 후 그 공기를 기도 속으로 적절히 불어넣어야 한다.
- 그런 다음 처치자의 입을 환아의 입에서 떼고 심장 마사지(심장 압박)를 5번 연거푸 한다. 그 다음 또다시 공기를 크게 들이마신 후 전과 같은 요령으로 한번 인공호흡을 하고 그 다음 심장 마사지를 5번 한다. 다시 설명하면 인공호흡을 한 번(1번) 한 후 심장 마사지(심장 압축/Cardiac compression)를 5번 한다.
- 1분간 총 인공호흡의 횟수는 환아의 나이와 크기에 따라 다르나
- 1세 이전 영아에게는 1분에 20회,
- 돌 이후의 유아나 유아기 이후 아이에게는 1분에 15회 한다.
- 8세 이후 큰 아이나 성인인 경우 1분에 10~12회 한다.
- 처치자의 입을 환아의 입에만, 또는 입과 콧구멍 두 부위에 대고 공기를 불어넣은 후, 아이의 폐 속에서 공기가 저절로 흘러나오도록 처치자의 입을 환아의 입이나, 입과 콧구멍에서 완전히 뗀 다음 곧 바로 심장 마사지를 5번 연거푸 한다.
- 인공호흡을 할 때 신생아나 영아의 입과 코에다 너무 세게 공기를 불어넣으면 폐포가 터질 수 있다.
- 숨을 거의 쉬지 못하거나, 아주 쉬지 못했던 환아가 스스로 숨을 거의 정상적으로 쉴 때까지 기본 심폐 소생술을 계속한다.
- 기본 심폐 소생술을 효과적으로 하려면 한 사람 이상이 함께해야 한다. 그리고 더 필요한 치료와 처치를 해주어야 한다.
- 그래서 기본 심폐 소생술을 시작하는 동시에 의료 구급대원, 응급실, 단골 소아청소년과 의사 등으로 부터 전화응급 도움을 긴급히 받는다.
- 경우에 따라 구급차나 다른 적절한 교통수단으로 가장 가까이에 있는 적절한 병원 응급실로 데리고 간다.
- 인공호흡을 해 줄 때는 심장 마사지를 동시 하는 것이 일반적이다.
- 인공호흡을 시작할 때나 하는 중 환아의 콧구멍이나 입을 통해서 하기도 속으로 공기를 적절히 불어넣어도 공기가 기도 속으로 더 이상 들어가지 않거나,
- 보통 때 숨 쉴 때처럼 앞가슴이 올라갔다 내려갔다 하지 않으면 이물(異物)이 기도 속에있고 그 이물로 기도가 막히거나 구토 물 등으로 기도가 막혀 있을 가능성이 있다고 판단할 수 있다.
- 이런 경우, 하고 있던 인공호흡과 심장 마사지를 즉시 중지하고 입안에 이물이 있나 속히 체크해 볼 수 있다.
- 입안에 이물이 보이지 않고 숨을 계속 쉬지 않으면 인공호흡과 심장 마사지를 또 다시 시작하거나,
- 또는 환아의 양쪽 견갑골 사이 중간 부분을 손바닥으로 5번 정도 쳐서 기도 속 이물이나 기도 속 구토 물이 입안 속으로나 입 밖으로 나오도록 빨리 시도한다. 또다시 인공호흡과 심장마사지를 전과 같이 계속 진행한다.
- 그래도 기도 속 이물 등으로 처치자가 공기를 환아의 입이나 콧구멍 속을 통해 기도 속으로 불어넣을 수 없고 환아가 숨을 쉬지 못할 때는 앞가슴 밀기나 오목가슴 미는 기도 이물제거처치 법으로 기도 속의 이물이 입 밖으로 나오게 또다시 시도한다. 그 다음 인공호흡과 심장 마사지를 다시 시작한다.
- 1세 이전 영아의 경우에는 등치기와 가슴 밀기로 기도 내 이물을 입안이나 입 밖으로 나오게 하고
- 1세 이후 아이들의 경우, 오목 가슴 밀기로 기도 내 이물이 입안이나 입 밖으로 나오게 처치하는 것이 보통이다.
- 기도 속에 이물이 들어갔을 때 참조.
기본 심폐 소생술을 할 때 심장 마사지를 하는 법을 사진으로 보기

사진 257. 1. 목에서 경동맥이 뛰나 알아본다.
Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP

사진 258. 2. 팔꿈치의 앞 부위에서 상완동맥이 뛰나 맥박을 짚어 알아본다.
Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP

사진 259. 서혜부에 있는 대퇴동맥에서 맥이 뛰나 알아본다.
Copyrightⓒ 2011 John Sangwon Lee, MD., FAAP

사진 260. 가슴에서 심장이 뛰나 알아본다.
1~2초 내에 목이나 팔이나 서혜부에 있는 동맥에서 맥이 뛰나 알아보든지 또는 가슴에서 맥이 뛰나 심장이 뛰나 알아본다.
Copyrightⓒ 2011 John Sangwon Lee, MD., FAAP
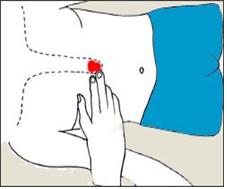
그림 261. 검상돌기가 있는 부위를 알아본다.
붉은 색으로 표시한 부분이 검상돌기이다.
Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP

사진 262. 검상돌기의 끝 부위를 알아본다.
검상돌기는 흉골의 맨 아래쪽에 있고 흉골의 일부이다. 심장 마사지는 흉골 아래 ⅓ 부분에서 한다.
Copyrightⓒ 2011 John Sangwon Lee, MD., FAAP

사진 263. 처치자의 한쪽 손바닥을 심장 마사지를 할 부위에 올려놓는다.
양쪽 젖꼭지를 잇는 횡선에서 한두 손가락의 넓이만큼 아래 부위, 검상돌기에서 한두 손가락 넓이만큼 위에 있는 흉골 부위에서 심장 마사지를 한다. 즉 심장 마사지는 흉골 아래 ⅓부분에서 한다.
Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP

사진 264.
1세 이하 영아들을 위해 심장 마사지를 할 때는 2~3개의 손가락을 이용해서 하고 매번 심장 마사지를 할 때마다 0.5~1인치 흉골 아래 ⅓ 부위를 눌러 심장 마사지를 한다.
1~8세 유아들이나 학령기 아이들을 위해 심장 마사지를 할 때는 손바닥으로 1~1.5인치 흉골 아래 ⅓ 부분을 눌러 한다. 그리고 8세까지 아이들을 위해 심장 마사지를 할 때는 1분에 100번,
8세 이상부터 성인을 위해서 심장 마사지를 할 때는 1분에 80~100번 한다.
Copyrightⓒ 2011 John Sangwon Lee, MD., FAAP

사진 265. 혼자만 있을 때는 처치자가 인공호흡도 하고 심장 마사지를 동시 하면서 도와줄 수 있는 사람을 큰 소리로 구한다.
Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP

사진 266. 두 사람 이상 있을 때는 한 사람은 인공호흡을 하고 다른 사람은 심장 마사지를 한다.
Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP

사진 267. 11. 처치자의 입을 환아의 입과 콧구멍, 두 부위에 대고 인공호흡을 하면서 도와줄 수 있는 사람을 큰 소리로 구한다.
Copyrightⓒ 2011 John Sangwon Lee, MD., FAAP

사진 268. 12. 두 사람 이상 있을 때는 한 사람은 인공호흡을 하고 다른 사람은 심장 마사지를 한다.
Copyright ⓒ 2011 John Sangwon Lee, MD, FAAP
Cardiopulmonary resuscitation(CPR)-2
First Aid Basic CPR
Table 41. Perform basic CPR to sustain life. 표 41. 생명을 유지하기 위해 기본 심폐 소생술을 한다.
| Basic CPR sequence |
1. Confirm that he is in an unresponsive state 2. Ask for help 3. Maintain a position capable of performing basic CPR and 4. Open the airway to secure the airway so that air can enter and exit the airway. 5. Check for apnea 6. Take 2 artificial respirations to blow air into the lungs and see if the chest rises up 7. It is common to start treatment with cardiac compression (extracorporeal (sex) cardiac compression) and perform general basic CPR. |
sources and references; Manual of emergency pediatrics 5th edition, Robert M. Reece, M.D.
1. Promptly assess and know if you are in respiratory arrest, in shock, in cardiac arrest and in respiratory arrest.
2. Then how soon should we know? Basic CPR to save life within 30 seconds to 1 minute You cannot save a life without first aid or specialized CPR first aid.
3. Determine if the airway is open to allow air to pass through or if the airway is blocked. Move the child to a safe place as possible and lay him flat on his back.
4. If possible, suck the secretions in the mouth or nasal passages (see www.drleepediatrics.com – Vol. 21 Home School Nursing for Children and Adolescents – Intake).
5. Check the following status.
o Are you breathing deeply?
o Whether the nostrils (nostrils/wings) flap with each breath,
o Does the chest or abdomen go up and down as you breathe?
o whether the muscles between the ribs are sucked into and out of the chest cavity; o What is your breathing rate,
o When you hold the patient’s ear close to the nostrils, check whether there is a sound of air coming out of the lungs.
o Are you breathing?
o If you have shortness of breath,
o Check to see if breathing has stopped.
6. Note the pulse, whether the pulse is beating, the number of pulses, whether the pulse is strong, slow, or irregular.
7. Check the blood circulation status by examining whether the skin color is pale or blue, whether the skin is cold or warm.
www.drleepediatrics.com – Refer to Vol. 8. Determine the patient’s level of conscious clarity. The level of conscious clarity is quickly assessed by whether it is agile, responds to words, responds to external painful stimuli, or has no response to such stimuli.
9. Remove all clothing to determine the cause of respiratory and cardiac arrest and perform CPR. Then, look for any signs of trauma.
10. It is important to quickly determine whether respiratory arrest and cardiac arrest are caused by airway obstruction, airway ventilation problems, or other problems.
• Recognize the symptoms 1 to 10 described above within 30 seconds or at least 1 minute, and then start the necessary treatment.
• It is not easy for doctors to recognize all these problems within 30 to 60 seconds. In addition, it is even more difficult for non-medical parents to find out all such information within 30 to 60 seconds.
• You also need to know that you are standing in the moment when you can and cannot save a life.
• If you learn more and know more about lifesaving information on a regular basis, you will be able to do basic cardiopulmonary resuscitation (CPR) to save lives more effectively.
Initiate life-sustaining basic CPR as follows.
• If the results of checking items 1 to 10 described above are summarized within 1 minute and it is determined that respiratory arrest and cardiac arrest have occurred, it is common to perform basic CPR in the following order to maintain life.
• Check for respiratory and cardiac arrest and
• Difficulty performing basic or advanced CPR properly on your own.
• Call out aloud someone who can help you out and ask for help.
• If possible, call urgently for help from a doctor, paramedic, emergency room, or ambulance at the same time.
• At the same time, in order to maintain the most appropriate position for basic CPR, lay the child on the back in a safe place. • Open the airway by turning the child’s face slightly to the side and raising the chin slightly upward. At this time, if there is any abnormality or trauma to the neck, do not turn, push, drag, or twist the neck without a doctor’s instruction.
• Put the patient’s ear close to the child’s mouth or nose and recheck that breathing is still in the state of breathing, whether breathing is heard, whether air is moving in and out of the airway (airway).
• After confirming that the patient is in respiratory arrest, put the operator’s mouth to the child’s mouth or nose, or both mouth and nose, and blow air into the child’s airways the first two times.
• At this time, check whether the chest rises upwards as if breathing normally.
• When the child’s airway is completely blocked by a foreign body, etc., it is normal for the pronotum to not rise upward because the air blown by the operator cannot enter the lungs due to the blocked airway.
• Check if the heart is beating or not by taking a pulse at the appropriate body part for your age.
• When performing artificial respiration for infants or small infants before 1 year of age, perform artificial respiration by placing the therapist’s mouth over the patient’s mouth and nose.
• When performing artificial respiration for infants after 1 year of age or school-age children, place the operator’s mouth on the patient’s mouth only, press the nasal flaps with your fingers, block both nostrils, and start artificial respiration.
• Simultaneously start a cardiac massage (cardiac compression).
• Provide artificial respiration with a ventilator when there is a medical device that can effectively perform CPR;
• Give artificial respiration using a respirator bag (breathing bag) and a mask.
• A more detailed description of advanced life support is omitted here.
• When performing CPR on infants before 1 year of age and infants and children under 8 years of age, give 20 breaths per minute and cardiac massage 100 times per minute.
• If the infant’s airway is blocked by a foreign body before the age of 1 year, when breathing stops and the heart stops, perform basic cardiopulmonary resuscitation and remove the foreign body from the airway by tapping the back area between the shoulders 5 times in a row with the palms. • Remove foreign objects from the airway by pushing the chest to remove foreign objects in the airway.
• When the airway of 1-8-year-old infants or school-age children is blocked by a foreign body and breathing stops and the heart stops, push the deep fossa (concave chest) with the palm of your hand toward the inside of the thoracic cavity 5 times to remove the foreign body from the airway.
• If a foreign body enters the airway of an infant 1-year-old or older or school-age child and is conscious, the Heimrik method or pushing the deep concave chest can remove the foreign body from the airway (refer to airway foreign body asphyxiation photo).
• Unable to say with certainty how long basic CPR should be performed to sustain life.
• Depending on the cause of respiratory arrest and cardiac arrest, it is common to require specialized CPR with other types of treatment, such as oxygen-breathing therapy.
• If possible, even basic cardiopulmonary resuscitation (CPR) to maintain life is ideally performed following the doctor’s emergency call treatment instructions.
It is normal to give 5 basic cardiac massages and 1 artificial respiration (see Figure 42).
Sources and References • Robert M. Reece, Manual Emergency Pediatrics, 4th Ed. p8
• Choking/CPR. AAP
A few more things to know when doing CPR
• When performing basic artificial respiration, it is decided whether to put the patient’s mouth only or the patient’s mouth to both the patient’s mouth and nostrils according to the child’s age and mouth size.
• Here, when the patient suddenly has difficulty breathing or barely breathing, artificial respiration is performed to supply oxygen to the child’s lungs by placing the patient’s mouth on the patient’s mouth or both the mouth and nostrils and blowing air directly into the child’s airway. How to do a cardiac massage (chest compression technique) is explained.
• Of both artificial respiration and heart massage, the priority is to give oxygen to the patient by performing artificial respiration first, and to open the airway before starting artificial respiration so that the air can flow through the airway well.
• If the airway is completely blocked, the air cannot enter the child’s lungs through the respiratory tract (airway), even if the caregiver blows air into the child through artificial respiration.
• Infectious diseases can cause respiratory and cardiac arrest.
• A person who performed basic CPR to maintain the life of a child who has respiratory and cardiac arrest due to an infectious disease may become infected with bacteria from the patient. After performing basic cardiopulmonary resuscitation (CPR), the patient should receive appropriate prophylactic antibiotic treatment according to the doctor’s recommendations.
• When an infant with respiratory and cardiac arrest is discovered due to sudden infant death, it is recommended that basic CPR be continued whenever possible until transported to a hospital capable of performing advanced CPR.
• If a foreign body is seen in the mouth of an unconscious, respiratory and cardiac arrest child, it is recommended to remove the foreign body with a finger or an appropriate medical device.
• Be aware that a foreign body in the pharyngeal cavity can go deeper into the lower airway next to it and block the lower airway more completely (see When a foreign body enters the airway).
• Depending on age, when performing basic cardiopulmonary resuscitation in children and adolescents, look at photos of artificial respiration with the patient’s mouth or the patient’s mouth and nose on the patient’s mouth
Photo 245. 1. Put the patient’s ear close to the child’s mouth or nostril and check if the patient is breathing. Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
Picture 246. 2. Observe whether the pronotum or abdomen moves up and down as you breathe, or place the operator’s hand on the patient’s pronotum to see if they breathe. Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
Picture 247. 3. The carotid artery is measured in the neck. It is common to check whether the pulse is in the brachial artery in the arm or the femoral artery in the groin in infants younger than 1 year of age, or in infants over 1 year of age or school-age children to determine whether the heart is beating by checking the vein in the carotid artery in the neck. to be. Or you can check your chest to see if your heart is beating. It shouldn’t take more than a second or two to recognize this. Learn to take your pulse on a regular basis. Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
Picture 248. 4. The brachial artery is counted. Within a second or two, see if your neck, arms, or groin are pulsing, or your heart is beating in your chest. Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
Picture 249. 5. Taking a pulse in the femoral artery Within a second or two, see if your neck, arms, or groin are pulsing, or your heart is beating in your chest. Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
Picture 250. 6. Again, check whether the heart is beating or breathing in the chest. Or, see if there is a pulse in the neck, arms, or groin. Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
Picture 251. 7. Open the airway to allow ventilation and good breathing. Put one hand of the caregiver on the forehead, tilt the child’s head back slightly, tilt the face and head slightly to the side, and raise the chin and face slightly with the other hand. Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
Picture 252. 8. Tilt your neck back slightly. The purpose of this treatment is to allow air to enter the airway well during artificial respiration as shown in the photo. This treatment is called airway securing. Copyrightⓒ 2011 John Sangwon Lee, MD., FAAP
Picture 253. 9. If there is secretions in the mouth or nasal passages, remove the secretions. It shouldn’t take more than 30 seconds to get to this point. Then, through the patient’s mouth, air is blown into the child’s mouth or through the mouth and nostrils into the airway. At first, blow air into airway #2, observing that the chest rises as if breathing normally. If the airway is completely obstructed, it is normal for the pronotum to not rise upwards when air is blown because air cannot enter the lungs. Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
Picture 254. 10. Blow air into the airway of an infant under 1 year of age or small infant by placing the patient’s mouth simultaneously on the mouth and nostrils. When performing mouth-to-mouth artificial respiration for infants over 1 year of age or school-age children, press the nose wing to close the nostrils with your fingers, and place the patient’s mouth on the patient’s mouth to start artificial respiration. Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
Photo 255. 11. When performing basic CPR on an older child 1 year old or older, place the operator’s mouth over the infant or school-age child’s mouth and blow air into the airway. At this time, block the nostrils with one hand. Copyrightⓒ 2011 John Sangwon Lee, MD., FAAP
Picture 256. 12. One caregiver puts the patient’s mouth only on the patient’s mouth or both the mouth and nostrils and blows air into the airway, while the other operator performs basic CPR by heart massage. Copyrightⓒ 2011 John Sangwon Lee, MD., FAAP
Artificial respiration by mouth
• The rescuer (caregiver) puts her ear close to the child’s mouth or nostrils and observes whether the child is breathing, and whether the forearm or abdomen moves upwards and downwards as it breathes, or the patient’s pronotum Place the operator’s hand on top and see if he is breathing or not.
• If it is determined that the child is breathing little or no breathing, start basic CPR immediately as follows.
• First, the airway is opened so that air can enter the alveoli through the nostrils → nasal passages, mouth, pharynx → larynx → trachea → bronchi. This treatment is called securing the airway.
• Put one hand on the child’s forehead, tilt the head slightly, place the other hand under the child’s chin, and lift the chin slightly upward to open the airway in the pharynx and open the airway such as the larynx, trachea, and bronchi. do.
• At this time, be careful not to block the pharyngeal airway by pulling the tongue and root of the tongue back into the pharyngeal cavity.
• As much as possible, keep the head, face and neck in this position during artificial respiration.
• However, you should never move your neck carelessly if you have or suspect that your cervical vertebrae are damaged.
• Depending on the size and age of the child, artificial respiration should be performed by placing the operator’s mouth only on the patient’s mouth, or on both the mouth and nostrils.
• Continue basic CPR until the hospital initiates CPR, or until it is determined that basic CPR is no longer necessary.
• When performing basic cardiopulmonary resuscitation for small children such as newborns and infants, blow air into the mouth and nostrils of the newborn or infant through the mouth of the operator.
• The person giving artificial respiration should also inhale an appropriate amount of air according to the age and size of the child, then open the mouth wide and blow air into the airway through the mouth and nostrils of the newborn or infant.
• When giving artificial respiration to an infant or school-age child after birth, close both nostrils by squeezing the patient’s two nose wings (nostrils) with the patient’s two fingers, and then press the patient’s mouth to the patient’s mouth and pass through the patient’s mouth. Blow air into the airways.
• After inhaling an appropriate amount of air, the operator should properly inhale the air into the airway so that the child’s chest rises and falls as in normal breathing.
• Then, remove the patient’s mouth from the child’s mouth and perform cardiac massage (cardiac compression) 5 times in succession. After that, take another big breath in the air, perform artificial respiration once again in the same way as before, and then do a heart massage 5 times. In other words, after giving 1 artificial respiration (1 time), cardiac massage (cardiac compression) is performed 5 times.
• The number of total ventilations per minute depends on the age and size of the child. o 20 times per minute for infants before 1 year of age; o 15 times per minute for infants after the age of birth or for children after infancy. o For older children or adults after the age of 8, do 10 to 12 times per minute.
• After blowing the patient’s mouth into the child’s mouth only or into both the mouth and nostrils, remove the patient’s mouth completely from the child’s mouth, mouth and nostrils to allow air to spontaneously flow out of the child’s lungs Immediately afterward, do a heart massage five times in a row.
• When giving artificial respiration, blowing too hard into the mouth and nose of a newborn or infant can cause the alveoli to burst.
• Continue basic cardiopulmonary resuscitation (CPR) until the child with little or no breathing is breathing almost normally on his/her own.
• Basic CPR requires more than one person to be effective. And more necessary treatment and treatment should be given.
• So, at the same time as starting basic CPR, get emergency telephone help from medical paramedics, emergency rooms, and regular pediatricians.
• If necessary, take them to the nearest appropriate hospital emergency room by ambulance or other suitable means of transportation.
• When giving artificial respiration, it is common to perform cardiac massage at the same time.
• No more air enters the airways when adequate air is blown into the lower respiratory tract through the child’s nostrils or mouth at the beginning or during artificial respiration;
• If the chest does not go up and down like normal breathing, it can be judged that there is a foreign object in the airway and there is a possibility that the airway is blocked by the foreign body or the airway is blocked by vomit.
• In this case, you can immediately stop artificial respiration and heart massage and check your mouth for foreign objects.
• If there is no visible foreign body in the mouth and breathing is not continued, start artificial respiration and cardiac massage again, or
• Alternatively, tap the middle part between the shoulder blades of the child about 5 times with the palm of your hand to quickly try to get foreign objects or vomit from the airway into or out of the mouth. Again, artificial respiration and cardiac massage continue as before.
• However, if the patient cannot breathe air through the mouth or nostrils of the patient and the patient is unable to breathe due to a foreign object in the airway, etc. Try again to get it out of your mouth. Then start artificial respiration and cardiac massage again.
• In the case of infants before the age of 1 year, push the back and chest to get the foreign object out of the mouth
• For children after 1 year of age, it is common to treat the foreign body in the mouth or out of the mouth by pushing the concave chest.
• See when a foreign object enters the airway. See
Photos of how to do heart massage during basic CPR
Picture 257.1. Recognize whether the carotid artery in the neck jumps. Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
Photo 258. 2. The brachial artery jumps in the front part of the elbow, so check the pulse. Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
Picture 259. Check if the pulse is beating in the femoral artery in the groin. Copyrightⓒ 2011 John Sangwon Lee, MD., FAAP
Picture 260. Check if the heart is beating in the chest. Within a second or two, detect whether an artery in the neck, arm, or groin is beating, or if the heart is beating or beating in the chest. Copyrightⓒ 2011 John Sangwon Lee, MD., FAAP
Figure 261. Recognize the area with the xiphoid process. The part marked in red is the sphenoid process. Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
Picture 262. Recognize the tip of the geomsang process. The xiphoid process is at the bottom of the sternum and is part of the sternum. Cardiac massage is performed in the lower third of the sternum. Copyrightⓒ 2011 John Sangwon Lee, MD., FAAP
Picture 263. Place one palm of the practitioner on the area to be massaged. Do a heart massage in the area below the width of one or two fingers on the horizontal line connecting both nipples, and in the sternum above the xiphoid process as much as one or two fingers wide. That is, the heart massage is done in the ⅓ part below the sternum. Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
Picture 264. For infants under one year of age, use two or three fingers to massage the heart, and with each heart massage, press the ⅓ area below the sternum by 0.5 to 1 inch. For heart massages for infants 1-8 years of age or school-age children, use the palm of your hand to press one-third of the way below the sternum by 1-1.5 inches. And 100 times a minute for heart massage for children up to 8 years old. For adults from 8 years of age and older, do 80 to 100 times a minute for heart massage. Copyrightⓒ 2011 John Sangwon Lee, MD., FAAP
Photo 265. When alone, the therapist provides artificial respiration and a heart massage at the same time, shouting for someone to help. Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
Photo 266. When there are more than one person, one person performs artificial respiration and the other performs heart massage. Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
Picture 267. 11. Place the patient’s mouth on the patient’s mouth and nostrils, and give artificial respiration, loudly asking for someone to help. Copyrightⓒ 2011 John Sangwon Lee, MD., FAAP
Picture 268. 12. When there are more than one person, one person performs artificial respiration and the other performs heart massage. Copyright ⓒ 2011 John Sangwon Lee, MD, FAAP
출처 및 참조 문헌 Sources and references
- NelsonTextbook of Pediatrics 22ND Ed
- The Harriet Lane Handbook 22ND Ed
- Growth and development of the children
- Red Book 32nd Ed 2021-2024
- Neonatal Resuscitation, American Academy Pediatrics
- www.drleepediatrics.com 제1권 소아청소년 응급 의료
- www.drleepediatrics.com 제2권 소아청소년 예방
- www.drleepediatrics.com 제3권 소아청소년 성장 발육 육아
- www.drleepediatrics.com 제4권 모유,모유수유, 이유
- www.drleepediatrics.com 제5권 인공영양, 우유, 이유식, 비타민, 미네랄, 단백질, 탄수화물, 지방
- www.drleepediatrics.com 제6권 신생아 성장 발육 육아 질병
- www.drleepediatrics.com제7권 소아청소년 감염병
- www.drleepediatrics.com제8권 소아청소년 호흡기 질환
- www.drleepediatrics.com제9권 소아청소년 소화기 질환
- www.drleepediatrics.com제10권. 소아청소년 신장 비뇨 생식기 질환
- www.drleepediatrics.com제11권. 소아청소년 심장 혈관계 질환
- www.drleepediatrics.com제12권. 소아청소년 신경 정신 질환, 행동 수면 문제
- www.drleepediatrics.com제13권. 소아청소년 혈액, 림프, 종양 질환
- www.drleepediatrics.com제14권. 소아청소년 내분비, 유전, 염색체, 대사, 희귀병
- www.drleepediatrics.com제15권. 소아청소년 알레르기, 자가 면역질환
- www.drleepediatrics.com제16권. 소아청소년 정형외과 질환
- www.drleepediatrics.com제17권. 소아청소년 피부 질환
- www.drleepediatrics.com제18권. 소아청소년 이비인후(귀 코 인두 후두) 질환
- www.drleepediatrics.com제19권. 소아청소년 안과 (눈)질환
- www.drleepediatrics.com 제20권 소아청소년 이 (치아)질환
- www.drleepediatrics.com 제21권 소아청소년 가정 학교 간호
- www.drleepediatrics.com 제22권 아들 딸 이렇게 사랑해 키우세요
- www.drleepediatrics.com 제23권 사춘기 아이들의 성장 발육 질병
- www.drleepediatrics.com 제24권 소아청소년 성교육
- www.drleepediatrics.com 제25권 임신, 분만, 출산, 신생아 돌보기
- Red book 29th-31st edition 2021
- Nelson Text Book of Pediatrics 19th- 21st Edition
- The Johns Hopkins Hospital, The Harriet Lane Handbook, 22nd edition
- 응급환자관리 정담미디어
- Pediatric Nutritional Handbook American Academy of Pediatrics
- 소아가정간호백과–부모도 반의사가 되어야 한다, 이상원 저
- The pregnancy Bible. By Joan stone, MD. Keith Eddleman, MD
- Neonatology Jeffrey J. Pomerance, C. Joan Richardson
- Preparation for Birth. Beverly Savage and Dianna Smith
- 임신에서 신생아 돌보기까지. 이상원
- Breastfeeding. by Ruth Lawrence and Robert Lawrence
- Sources and references on Growth, Development, Cares, and Diseases of Newborn Infants
- Emergency Medical Service for Children, By Ross Lab. May 1989. p.10
- Emergency care, Harvey Grant and Robert Murray
- Emergency Care Transportation of Sick and Injured American Academy of Orthopaedic Surgeons
- Emergency Pediatrics A Guide to Ambulatory Care, Roger M. Barkin, Peter Rosen
- Quick Reference To Pediatric Emergencies, Delmer J. Pascoe, M.D., Moses Grossman, M.D. with 26 contributors
- Neonatal resuscitation Ameican academy of pediatrics
- Pediatric Nutritional Handbook American Academy of Pediatrics
- Pediatric Resuscitation Pediatric Clinics of North America, Stephen M. Schexnayder, M.D.
-
Pediatric Critical Care, Pediatric Clinics of North America, James P. Orlowski, M.D.
-
Preparation for Birth. Beverly Savage and Dianna Smith
-
Infectious disease of children, Saul Krugman, Samuel L Katz, Ann A.
- 제4권 모유, 모유수유, 이유 참조문헌 및 출처
- 제5권 인공영양, 우유, 이유, 비타민, 단백질, 지방 탄수 화물 참조문헌 및 출처
- 제6권 신생아 성장발육 양호 질병 참조문헌 및 출처
- 소아과학 대한교과서
Copyright ⓒ 2014 John Sangwon Lee, MD., FAAP
“부모도 반의사가 되어야 한다”-내용은 여러분들의 의사로부터 얻은 정보와 진료를 대신할 수 없습니다.
“The information contained in this publication should not be used as a substitute for the medical care and advice of your doctor. There may be variations in treatment that your doctor may recommend based on individual facts and circumstances.
“Parental education is the best medicine.